
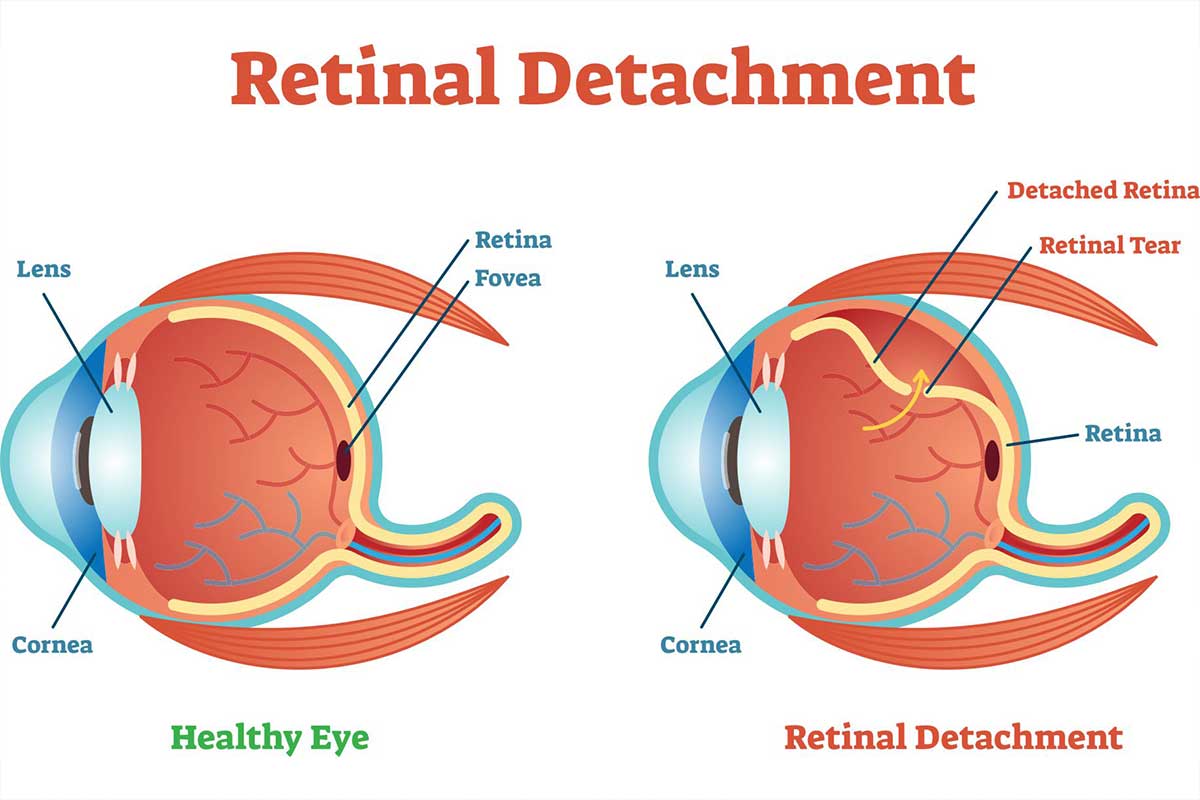
Normal vision
The retina is a thin membrane which is attached to the back surface of the eye and acts much like the film in a camera. When light enters the eye, it passes through the cornea and lens and is focused onto the retina. The retina transforms the light energy into vision and sends the information back to the brain through the optic nerve.
In order to function properly, the retina must be nourished by a layer behind it – the choroid.
Retinal Detachment
In retinal detachment, the retina peels away from the choroid and floats in the vitreous cavity, thus losing its function. If not treated early, retinal detachment may lead to impairment or complete loss of vision.
Cause
Most retinal detachments are preceded by one or more tears or holes in the retina. Tears are usually caused by traction exerted on the retina by strands in the vitreous body. Some of the fluid that fills the interior of the eye passes through these openings and undermines the retina, producing its separation from the choroid.
A combination of factors are usually responsible for retinal detachment. The vitreous, which fills most of the volume of the eye, tends to shrink with age. If a cataract has been removed, this shrinkage is accelerated. If the retina is thin because of age, high myopia, injury or hereditary factors, the pull of the shrinking vitreous may produce retinal tears, which in turn may progress to retinal detachment.
It should be noted that there are some retinal detachments that are caused by other diseases in the eye such as tumours, severe inflammations or complications of diabetes. These so called secondary detachments do not have tears or holes in the retina and treatment of the disease which caused the retinal detachment is the only treatment which may allow the retina to return to its normal position.
Symptoms
Middle-aged and older persons may see floating black spots or flashes of light in their vision. (These are usually less common in children or young adults). In most cases, these symptoms do not indicate serious problems. However, in some eyes, the sudden appearance of spots or flashes of light may indicate substantial shrinkage of the vitreous with tears in the retina. A comprehensive medical eye examination by an ophthalmologist is necessary to check the inside of the eye to determine if retinal tears are present. Such an examination is desirable as soon as symptoms develop because fresh retinal tears may be treatable by laser photocoagulation before they lead to a more serious retinal detachment. Some retinal detachments may begin without noticeable floaters or light flashes.
In those instances, patients may notice a wavy or watery quality in their overall vision or the appearance of a dark shadow in some part of their vision. Further development of the retinal detachment will blur central vision and create significant sight loss in one eye unless the detachment is repaired.
Some detachments may occur suddenly and the patient will experience a total loss of vision in one eye. Similar rapid loss of vision may also be caused by bleeding into the vitreous area of the eye which may happen when the retina is torn.
Treatment
Prompt treatment is essential. Successful reattachment of the retina consists of sealing the retinal tear and preventing the retina from pulling away from the back of the eye again. There are several procedures that may be used. The choice depends on the severity of the retinal detachment and the judgment of the ophthalmologist.
Laser Photocoagulation: When new small retinal tears are found with little or no nearby retinal detachment, the tears are sometimes sealed with a laser light. The laser places small burns around the edge of the tear. These produce scars that seal down the edges of the tear and prevent fluid from passing through and collecting under the retina.
Freezing (Cryopexy): Freezing the back wall of the eye behind a retinal tear will also stimulate scar formation and seal down the edges.
Surgical repair: Such operations vary depending on the extent of the detachment and resulting damage, but each is designed to press the wall of the eye against the retinal holes, holding both tissues together until scarring seals the tears. Sometimes fluid must be drained from under the retina to allow it to settle back onto the eye wall. Often a silicone band or pressure pad is placed on the outside of the eye to gently push the back wall of the eye against the retina.
In more complex retinal detachments, it may be necessary to use a technique called vitrectomy. This operation cuts the connected bands of vitreous away from the retina and removes the shrunken vitreous body from the eye. In some cases, when the detached retina itself is severely shrunken and puckered, it may have to be pushed back to the wall of the eye by temporarily placing the vitreous cavity with air or gas. Eventually, clear fluid from the blood seeps into this space to fill it permanently.
Prognosis
Over 90% of all retinal detachments can be reattached by modern surgical techniques. Occasionally, more than one operation may be required.
If the retina is successfully reattached, the eye will retain some degree of sight, and blindness will be prevented. However, the degree of vision which finally returns about six months after successful surgery, depends on a number of factors. In general, there is less visual return when the retina has been detached for a long duration, or if there is a fibrous growth on the surface of the retina.
Approximately 40% of successfully treated retinal detachments achieved excellent vision. The remainder attain varying amounts of reading and/or travelling vision. Unfortunately, due to continuous shrinkage of the vitreous and the development of fibrous growths on the retina, not all retinas can be reattached.